Difference between revisions of "The logic of classical language/pt"
(Created page with "A linguagem dos predicados é expressa da seguinte maneira") |
(Created page with "Neste ponto, também deve ser considerado que a lógica dos predicados não é usada apenas para provar que um conjunto particular de premissas implica uma evidência particular") |
||
| Line 594: | Line 594: | ||
<math>\{a \in x \mid \forall \text{x} \; A(\text{x}) \rightarrow {B}(\text{x}) \vdash A( a)\rightarrow B(a) \}</math>. <math>(1)</math> | <math>\{a \in x \mid \forall \text{x} \; A(\text{x}) \rightarrow {B}(\text{x}) \vdash A( a)\rightarrow B(a) \}</math>. <math>(1)</math> | ||
| − | + | Neste ponto, também deve ser considerado que a lógica dos predicados não é usada apenas para provar que um conjunto particular de premissas implica uma evidência particular <math>(1)</math>. It is also used to prove that a particular assertion is not true, or that a particular piece of knowledge is logically compatible/incompatible with a particular evidence. | |
In order to prove that this proposition is true we must use the above mentioned<u>demonstration by absurdity</u>. If its denial creates a contradiction, surely the dentist's proposition will be true: | In order to prove that this proposition is true we must use the above mentioned<u>demonstration by absurdity</u>. If its denial creates a contradiction, surely the dentist's proposition will be true: | ||
Revision as of 16:09, 3 November 2021

Concluindo, fica evidente que uma lógica clássica da linguagem, que tem uma abordagem extremamente dicotômica (ou algo é branco ou é preto), não consegue descrever os muitos matizes que apresentam as situações clínicas reais..
Como veremos em breve, este artigo mostrará que a lógica clássica carece da precisão necessária, obrigando-nos a aprimorá-la com outros tipos de linguagens lógicas..
Introdução
Nós separamos no capítulo anterior sobre ' Lógica da linguagem médica' em uma tentativa de mudar a atenção do sintoma clínico ou sinal para a linguagem de máquina criptografada para a qual, os argumentos de Donald E Stanley , Daniel G Campos e Pat Croskerry são bem-vindos, mas ligados ao tempo como portador de informação (antecipação do sintoma) e à mensagem como linguagem de máquina e não como linguagem não verbal).[1][2]
Obviamente, isso não exclui a validade da história clínica construída sobre uma linguagem verbal pseudo-formal já bem enraizada na realidade clínica e que já provou sua autoridade diagnóstica.. A tentativa de desviar a atenção para uma linguagem de máquina e para o Sistema fornece nada além de uma oportunidade para a validação da Ciência Médica Diagnóstica.

Estamos definitivamente cientes de que nosso Linux Sapiens ainda está perplexo com o que foi antecipado e continua a se perguntar

(um pouco de paciencia por favor)
Não podemos fornecer uma resposta convencional porque a ciência não avança com afirmações que não são justificadas por perguntas e reflexões cientificamente validadas; e é justamente por isso que tentaremos dar voz a algumas reflexões, perplexidades e dúvidas expressas sobre alguns temas básicos trazidos à discussão em alguns artigos científicos..
Um desses tópicos fundamentais é 'Biologia Craniofacial'.
Vamos começar com um estudo bem conhecido de Townsend e Brook[3]: neste trabalho, os autores questionam o status quo da pesquisa fundamental e aplicada em 'Biologia Craniofacial' para extrair considerações clínicas e implicações. Um dos tópicos que abordaram foi a "Abordagem Interdisciplinar", na qual Geoffrey Sperber e seu filho Steven viram a força do progresso exponencial da 'Biologia Craniofacial' em inovações tecnológicas como sequenciamento de genes, tomografia computadorizada, ressonância magnética, varredura a laser, análise de imagens , ultrassonografia e espectroscopia[4].
Outro tópico de grande interesse para a implementação da 'Biologia Craniofacial' é a consciência de que os sistemas biológicos são 'Sistemas Complexos'[5] e que a 'epigenética' desempenha um papel fundamental na biologia molecular craniofacial. Pesquisadores de Adelaide e Sydney fornecem uma revisão crítica no campo da epigenética voltada, de fato, para as disciplinas odontológicas e craniofaciais.[6] A fenômica, em particular, discutida por esses autores (ver Phenomics)) é um campo de pesquisa geral que envolve a medição das mudanças nos dentes e estruturas orofaciais associadas resultantes das interações entre genética, epigenética e ambiente fatores durante o desenvolvimento.[7] Nesse mesmo contexto, o trabalho de Irma Thesleff de Helsinque, Finlândia, merece destaque.. Ela explica em seu trabalho que há uma série de centros de sinalização transitórios no epitélio dentário que desempenham papéis importantes no programa de desenvolvimento dentário..[8] Além disso, existem outros trabalhos, de Peterkova R, Hovor akova M, Peterka M, Lesot H, fornecendo uma revisão fascinante dos processos que ocorrem durante o desenvolvimento dentário;[9][10][11] para fins de completude, não vamos esquecer os trabalhos de Han J, Menicanin D, Gronthos S e Bartold PM., que revisam a documentação abrangente sobre células-tronco, engenharia de tecidos e regeneração periodontal.[12]
Nesta revisão, argumentos não poderiam faltar sobre as influências genéticas, epigenéticas e ambientais durante a morfogênese que levam a variações no número, tamanho e formato do dente.[13][14] e a influência da pressão da língua no crescimento e função craniofacial.[15][16]
O trabalho extraordinário de Townsend e Brook também merece uma menção[3], e o conteúdo intrínseco do que foi relatado nele combina igualmente bem com outro autor louvável: HC Slavkin.[17] Slavkin afirma que:
- "O futuro está cheio de oportunidades significativas para melhorar os resultados clínicos de malformações craniofaciais congênitas e adquiridas. Os médicos desempenham um papel fundamental, pois o pensamento crítico e o público clínico melhoram substancialmente a precisão do diagnóstico e, portanto, os resultados clínicos da saúde."
(Vou te dar um exemplo prático)
No capítulo "Introdução" colocamos algumas questões sobre o tema da má oclusão, mas neste contexto simulamos a lógica da linguagem médica do dentista diante do caso clínico apresentado no "Capítulo de introdução" com suas conclusões diagnósticas e terapêuticas.
O paciente tem uma mordida cruzada unilateral posterior e uma mordida aberta anterior.[18] A mordida cruzada é outro elemento perturbador da oclusão normal[19] para o qual é obrigatório tratado juntamente com a mordida aberta.[20][21] Este tipo de raciocínio significa que o modelo (sistema mastigatório) é 'normalizado para oclusão'; e lido ao contrário, significa que a discrepância oclusal é a causa da má oclusão, portanto, uma doença do Sistema Mastigatório, e portanto uma intervenção para restaurar a função mastigatória fisiológica é justificável. (Figura 1a).
Este exemplo é a Lógica Clássica, como iremos explicar em detalhes, mas agora surge uma dúvida:
- Na época em que os axiomas ortodônticos e ortognáticos estavam construindo protocolos confirmados pela Comunidade Científica Internacional, eles sabiam das informações que discutimos na introdução deste capítulo?
Certamente não porque o tempo ' seja o portador da informação' , mas apesar deste limite cognitivo, procedemos com uma Lógica Clássica muito questionável para a segurança do cidadão.
(claro, mas a sequência lógica já foi antecipada)
Se o mesmo caso fosse interpretado com uma mentalidade que seguisse uma 'lógica da linguagem do sistema' (ela será discutida no capítulo apropriado), as conclusões seriam surpreendentes.
Se observarmos as respostas eletrofisiológicas realizadas no paciente com má oclusão nas figuras 1b, 1c e 1d (com a explicação feita diretamente na legenda para simplificar a discussão), notaremos que esses dados podem nos fazer pensar em qualquer coisa exceto uma 'Maloclusão 'e, portanto, os axiomas do tipo ortodôntico e ortognático' causa / efeito 'deixam um vazio conceitual.

Figura 1a: Paciente com má oclusão, mordida aberta e mordida cruzada posterior direita que em termos de reabilitação deve ser tratado com terapia ortodôntica e / ou cirurgia ortognática
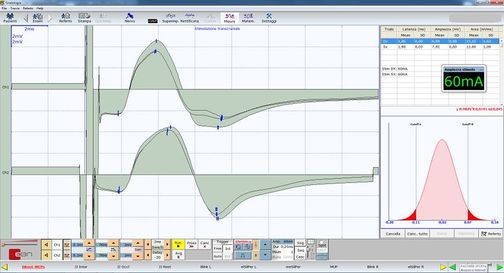
Figura 1b: Potencial evocado motor da estimulação elétrica transcraniana das raízes do trigêmeo. Observe a simetria estrutural calculada pela amplitude pico a pico nos masseters direito e esquerdo.
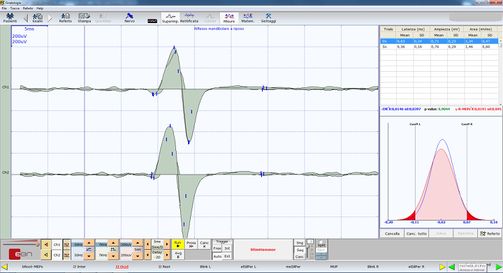
Figura 1c: Reflexo mandibular evocado ou empurrão da mandíbula pela percussão do queixo por meio de um martelo neurológico acionado. Observe a simetria funcional calculada pela amplitude de pico a pico nos masseters esquerdo e direito (traços superior e inferior, respectivamente)
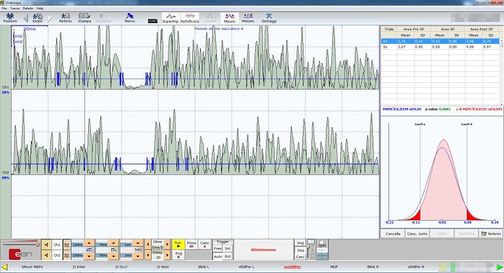
Figura 1d: Período de silêncio mecânico evocado por percussão do queixo por meio de um martelo neurológico acionado. Observe a simetria funcional calculada na área integral dos masseters direito e esquerdo..



(Faremos isso seguindo o caso clínico de nossa Mary Poppins)
Formalismo matemático
Neste capítulo, iremos reconsiderar o caso clínico da infeliz Mary Poppins sofrendo de Dor Orofacial por mais de 10 anos, quando seu dentista diagnosticou 'Desordens Temporomandibulares' (DTMs) ou melhor, Dor Orofacial por DTMs. Para entender melhor por que a formulação diagnóstica exata permanece complexa com uma Lógica da Linguagem Clássica, devemos entender o conceito no qual a filosofia da linguagem clássica se baseia com uma breve introdução ao tema..
Proposições
A lógica clássica é baseada em proposições. Costuma-se dizer que uma proposição é uma sentença que pergunta se a proposição é verdadeira ou falsa. Na verdade, uma proposição em matemática geralmente é verdadeira ou falsa, mas isso é obviamente um pouco vago demais para ser uma definição. Pode ser tomado, na melhor das hipóteses, como um aviso: se uma frase, expressa em linguagem comum, não faz sentido perguntar se é verdadeira ou falsa, não será uma proposição, mas outra coisa.
Pode-se argumentar se as sentenças de linguagem comum são proposições ou não, pois em muitos casos não é frequentemente evidente se uma determinada afirmação é verdadeira ou falsa.
‘Felizmente, as proposições matemáticas, se bem expressas, não mostram tais ambigüidades’.
As proposições mais simples podem ser combinadas entre si para formar proposições novas e mais complexas. Isso ocorre com a ajuda de operadores chamados operadores lógicos e conectivos de quantificação que podem ser reduzidos ao seguinte[22]:
- Conjunção, que é indicado pelo símbolo (and):
- Disjunção, que é indicado pelo símbolo (or):
- Negação, que é indicado pelo símbolo (not):
- Implicação, que é indicado pelo símbolo (if ... then):
- Consequência, que é indicado pelo símbolo (is a partition of..):
- Quantificador universal, que é indicado pelo símbolo (for all):
- Demonstração, que é indicado pelo símbolo (such that): and
- Filiação, que é indicado pelo símbolo (is an element of) ou pelo símbolo (is not an element of):









Demonstração por absurdo
Além disso, na lógica clássica, existe um princípio denominado terceiro excluído , que declara que uma frase que não pode ser falsa deve ser considerada verdadeira, uma vez que não existe uma terceira possibilidade.
Suponha que precisamos provar que a proposição é verdadeira. O procedimento consiste em mostrar que a suposição de que é falsa leva a uma contradição lógica. Assim, a proposição não pode ser falsa e, portanto, de acordo com a lei do terceiro excluído, deve ser verdadeira. Este método de demonstração é chamado de demonstração por absurdo [23]

Predicados
O que descrevemos brevemente até agora é a lógica das proposições. Uma proposição afirma algo sobre objetos matemáticos específicos, como: '2 é maior que 1, então 1 é menor que 2' ou 'um quadrado não tem 5 lados, então um quadrado não é um pentágono'. Muitas vezes, no entanto, os enunciados matemáticos não se referem a um único objeto, mas a objetos genéricos de um conjunto, como: ' têm mais de 2 metros de altura' Onde denota um grupo genérico (por exemplo, todos os jogadores de voleibol). Neste caso, falamos de predicados.

Intuitivamente, um predicado é uma frase relativa a um grupo de elementos (que em nosso caso médico serão os pacientes) e que afirma algo sobre eles.
(vamos ver o que a Lógica da Linguagem Clássica nos diz)
Além das confirmações derivadas da lógica da linguagem médica discutida no capítulo anterior, o colega dentista adquire outros dados instrumentais que lhe permitem confirmar seu diagnóstico. Os últimos testes referem-se à análise dos traços axiográficos usando uma embreagem paraoclusal funcional personalizada que permite a visualização e quantificação dos traços condilares nas funções mastigatórias.. Como pode ser visto na Figura 4 o achatamento dos traços condilares do lado direito tanto na cinética mastigatória mediotrusiva (cor verde) e os ciclos de abertura e protrusão (cor cinza) confirmam o achatamento anatômico e funcional da ATM direita na dinâmica mastigando. Além da axiografia, o colega realiza uma eletromiografia de superfície nos masseteres (fig. 6) solicitando que o paciente exerça o máximo de força muscular. Este tipo de análise eletromiográfica é denominado "Padrão Interferencial EMG" devido ao conteúdo de alta frequência dos picos que sofrem interferência de fase. De fato, a Figura 6 mostra uma assimetria no recrutamento das unidades motoras do masseter direito (traço superior) em relação ao masseter esquerdo (traço inferior).[24][25][26][27]
Segunda Abordagem Clínica
(passe o mouse sobre as imagens)

Figura 2: Paciente relatando 'dor orofacial' na face hemilateral direita

Figura 3: Estratigrafia da ATM do paciente mostrando sinais de achatamento condilar e osteófito

Figura 4: Tomografia Computadorizada da ATM
Figura 5: Axiografia do paciente mostrando um achatamento do padrão de mastigação no côndilo direito
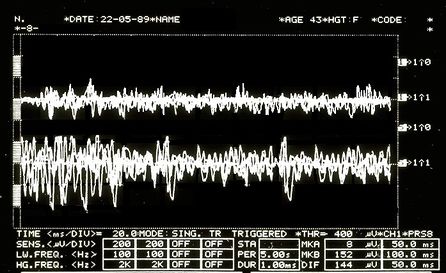
Figura 6: Padrão Interferencial EMG. Traços superiores sobrepostos correspondentes ao masseter direito, inferiores ao masseter esquerdo.




Proposições dentais
Ao buscar usar o formalismo matemático para traduzir as conclusões a que chega o dentista com a linguagem da lógica clássica, consideramos os seguintes predicados:
- x Pacientes normais (normal significa pacientes comumente presentes no ambiente especializado)

- Remodelação óssea com osteófito a partir de exame estratigráfico e tomografia computadorizada condilar; e
- Desordens Temporomandibulares (DTMs) resultando em Dor Orofacial (OP)
- Paciente específico: Mary Poppins



Qualquer paciente normal quem é positivo no exame radiográfico da ATM [Figura 2 e 3] é afetado por TMDs ; Disto segue que sendo Mary Poppins positiva (e também sendo uma paciente "normal") no raio-x da ATM então Mary Poppins também é afetada por TMDs





A linguagem dos predicados é expressa da seguinte maneira:
.


Neste ponto, também deve ser considerado que a lógica dos predicados não é usada apenas para provar que um conjunto particular de premissas implica uma evidência particular . It is also used to prove that a particular assertion is not true, or that a particular piece of knowledge is logically compatible/incompatible with a particular evidence.
In order to prove that this proposition is true we must use the above mentioneddemonstration by absurdity. If its denial creates a contradiction, surely the dentist's proposition will be true:
.


"" states that it is not true that those who test positive on TMJ CT have TMDs, so Mary Poppins (TMJ CT positive normal patient) does not have TMDs.
The dentist believes that Mary Poppins' claim (that she does not have TMD under these premises) is a contradiction so the main claim is true.
Neurophysiological proposition
Let us imagine that the neurologist disagrees with the conclusion and asserts that Mary Poppins is not affected by TMDs or that at least it is not the main cause of Orofacial Pain, but that, rather, she is affected by a neuromotor Orofacial Pain (nOP), therefore that she does not belong to the group of 'normal patients' but is to be considered a 'non-specific patient' (uncommon in the specialist context).
Obviously, this dialectic would last indefinitely because both would defend their scientific-clinical context; but let us see what happens in the logic of predicates.
The neurologist's statement would be like:
.


"" means that every patient who is TMJ CT positive has TMDs but even though Mary Poppins is TMJ CT positive, she does not have TMDs.
In order to prove that this proposition is true, we must use once again the above mentioned demonstration by absurdity. If its denial creates a contradiction, surely the neurologist's proposition will be true:
.


Following the logical rules of predicates, there is no reason to say that denial (4) is contradictory or meaningless, therefore the neurologist (unlike the dentist) would not seem to have the logical tools to confirm his conclusion.
(don't take it for granted)
Compatibility and incompatibility of the statements
The complication lies in the fact that the dentist will present a series of statements as clinical reports such as the stratigraphy and CT of the TMJ, that indicate an anatomical flattening of the joint, axiography of the condylar traces with a reduction in kinematic convexity and a tracing EMG interference pattern in which an asymmetrical pattern on the masseters is highlighted. These assertions can easily be considered a contributing cause of the damage to the Temporomandibular Joint and, therefore, responsible for the 'Orofacial pain'.
Documents, reports and clinical evidence can be used to make the neurologist's assertion incompatible and the dentist's diagnostic conclusion compatible. To do this we must present some logical rules that describe the compatibility or incompatibility of the logic of classical language:
- A set of sentences , and a number of other phrases or statements are logically compatible if, and only if, the union between them is coherent.
- A set of sentences , and a number of other phrases or statements are logically incompatible if, and only if, the union between them is incoherent.




Let us try to follow this reasoning with practical examples:
The dentist colleague exposes the following sentence:
: Following the personalized techniques suggested by Xin Liang et al.[28] who focuses on the quantitative microstructural analysis of the fraction of the bone value, the trabecular number, the trabecular thickness and the trabecular separation on each slice of the CT scan of a TMJ, it appears that Mary Poppins is affected by Temporomandibular Disorders (TMDs) and the consequence causes Orofacial Pain.
At this point, however, the thesis must be confirmed with further clinical and laboratory tests, and in fact the colleague produces a series of assertions that should pass the compatibility filter as described above, namely:
Bone remodelling: The flattening of the axiographic traces highlighted in figure 5 indicates the joint remodelling of the right TMJ of Mary Poppins, such a report can be correlated to a series of researches and articles that confirm how malocclusion can be associated with morphological changes in the temporomandibular joints, particularly when combined with the age as the presence of a chronic malocclusion can worsen the picture of bone remodelling.[29] These scientific references determine the compatibility of the assertion.

Sensitivity and specificity of the axiographic measurement: A study was conducted to verify the sensitivity and specificity of the data collected from a group of patients affected by temporomandibular joint disorders with an ARCUSdigma axiographic system[30]; it confirmed a sensitivity of the 84.21% and a 92.86% sensitivity for the right and left TMJs respectively, and a specificity of 93.75% and 95.65%.[31] These scientific references determine compatibility of the assertion in the dental context precisely because of the consistency of related studies.[32]

Alteration of condylar paths: Urbano Santana-Mora and coll.[33] evaluated 24 adult patients suffering from severe chronic unilateral pain diagnosed as Temporomandibular Disorders (TMDs). The following functional and dynamic factors were evaluated:

- masticatory function;
- remodelling of the TMJ or condylar pathway (CP); and
- lateral movement of the jaw or lateral guide (LG).
The CPs were assessed using conventional axiography and LG was assessed by using kinesiograph tracing[34]; Seventeen (71%) of the 24 (100%) patients consistently showed a side of habitual chewing side. The mean and standard deviation of the CP angles was 47.90 9.24) degrees. The average of LG angles was 42.9511.78 degrees.
Data collection emerged from the conception of a new TMD paradigm in which the affected side could be the usual chewing side, the side where the mandibular lateral kinematic angle was flatter. This parameter may also be compatible with the dental claim.

EMG Intereference pattern: M.O. Mazzetto and coll.[35] showed that the electromyographic activity of the anterior temporal muscles and the masseter was positively correlated with the "Craniomandibular index", indiced (CMI) with a and suggesting that the use of CMI to quantify the severity of TMDs and EMG to assess the masticatory muscle function, may be an important diagnostic and therapeutic elements. These scientific references determine compatibility of the assertion.


?

Obviously, the dentist colleague could endlessly keep on casting his statements, indefinitely.
Well, all of these statements seem coherent with the sentence initially described, whereby the dentist colleague feels justified in saying that the set of sentences , and a number of other assertions or clinical data are logically compatible as the union between them is coherent.
(It would seem so!
But, be careful, only in his own dental context!)
This statement is so true that the could be infinitely extended, widened enough to obtain an that corresponds to it in an infinite significance, as long as it remains limited in its context; yet, without meaning anything from a clinical point of view in other contexts, like in the neurologist one, for instance.


Final considerations
From a perspective of observation of this kind, the Logic of Predicates can only fortify the dentist’s reasoning and, at the same time, strengthen the principle of the excluded third: the principle is strengthened through the compatibility of the additional assertions which grant the dentist a complete coherence in the diagnosis and in confirming the sentence : Poor Mary Poppins either has TMD, or she has not.
Basically, given the compatibility of the assertions , coherently saying that Orofacial Pain is caused by a Temporomandibular Disorders could become incompatible if another series of assertions were shown to be coherent: this would make a different sentence compatible : could poor Mary Poppins suffer from Orofacial Pain from a neuromotor disorder (nOP) and not by a Temporomandibular Disorders?

In the current medical language logic, such assertions only remain assertions, because the convictions and opinions do not allow a consequent and quick change of the mindset.
Moreover, taking into account the risk that this change entails, in fact, we might consider a recent article on the epidemiology of temporomandibular disorders[36] in which the authors confirm that despite the methodological and population differences, pain in the temporomandibular region appears to be relatively common, occurring in about the 10% of the population; we may then objectively be led to hypothesize that our Mary Poppins can be included in the 10% of the patients mentioned in the epidemiological study, and contextually be classified as a patient suffering from Orofacial Pain from Temporomandibular Disorders (TMDs).
In conclusion, it is evident that a classical logic of language, which has an extremely dichotomous approach (either it is white or it is black), cannot depict the many shades that occur in real clinical situations.
We need to find a more convenient and suitable language logic...
(perhaps)
- ↑ Stanley DE, Campos DG, «The logic of medical diagnosis», in Perspect Biol Med, 2013.
PMID:23974509
DOI:10.1353/pbm.2013.0019 - ↑ Croskerry P, «Adaptive expertise in medical decision making», in Med Teach, 2018.
PMID:30033794
DOI:10.1080/0142159X.2018.1484898 - ↑ 3.0 3.1 Townsend GC, Brook AH, «The face, the future, and dental practice: how research in craniofacial biology will influence patient care», in Aust Dent J, Australian Dental Association, 2014.
PMID:24646132
DOI:10.1111/adj.12157 - ↑ Sperber GH, Sperber SM, «The genesis of craniofacial biology as a health science discipline», in Aust Dent J, Australian Dental Association, 2014.
PMID:24495071
DOI:10.1111/adj.12131 - ↑ Brook AH, Brook O'Donnell M, Hone A, Hart E, Hughes TE, Smith RN, Townsend GC, «General and craniofacial development are complex adaptive processes influenced by diversity», in Aust Dent J, Australian Dental Association, 2014.
PMID:24617813
DOI:10.1111/adj.12158 - ↑ Williams SD, Hughes TE, Adler CJ, Brook AH, Townsend GC, «Epigenetics: a new frontier in dentistry», in Aust Dent J, Australian Dental Association, 2014.
PMID:24611746
DOI:10.1111/adj.12155 - ↑ Yong R, Ranjitkar S, Townsend GC, Brook AH, Smith RN, Evans AR, Hughes TE, Lekkas D, «Dental phenomics: advancing genotype to phenotype correlations in craniofacial research», in Aust Dent J, Australian Dental Association, 2014.
PMID:24611797
DOI:10.1111/adj.12156 - ↑ Thesleff I, «Current understanding of the process of tooth formation: transfer from the laboratory to the clinic», in Aust Dent J, 2013.
DOI:10.1111/adj.12102 - ↑ Peterkova R, Hovorakova M, Peterka M, Lesot H, «Three‐dimensional analysis of the early development of the dentition», in Aust Dent J, Wiley Publishing Asia Pty Ltd on behalf of Australian Dental Association, 2014.
DOI:10.1111/adj.12130 - ↑ Lesot H, Hovorakova M, Peterka M, Peterkova R, «Three‐dimensional analysis of molar development in the mouse from the cap to bell stage», in Aust Dent J, 2014.
DOI:10.1111/adj.12132 - ↑ Hughes TE, Townsend GC, Pinkerton SK, Bockmann MR, Seow WK, Brook AH, Richards LC, Mihailidis S, Ranjitkar S, Lekkas D, «The teeth and faces of twins: providing insights into dentofacial development and oral health for practising oral health professionals», in Aust Dent J, 2013.
DOI:10.1111/adj.12101 - ↑ Han J, Menicanin D, Gronthos S, Bartold PM, «Stem cells, tissue engineering and periodontal regeneration», in Aust Dent J, 2013.
DOI:10.1111/adj.12100 - ↑ {{Cite book | autore = Brook AH | autore2 = Jernvall J | autore3 = Smith RN | autore4 = Hughes TE | autore5 = Townsend GC | titolo = The Dentition: The Outcomes of Morphogenesis Leading to Variations of Tooth Number, Size and Shape | url = https://onlinelibrary.wiley.com/doi/epdf/10.1111/adj.12160 | volume = | opera = Aust Dent J | anno = 2014 | editore = | città = | ISBN = | PMID = | PMCID = | DOI = 10.1111/adj.12160 | oaf = | LCCN = | OCLC =
- ↑ Seow WK, «Developmental defects of enamel and dentine: challenges for basic science research and clinical management», in Aust Dent J, 2014.
PMID:24164394
DOI:10.1111/adj.12104 - ↑ Kieser JA, Farland MG, Jack H, Farella M, Wang Y, Rohrle O, «The role of oral soft tissues in swallowing function: what can tongue pressure tell us?», in Aust Dent J, 2013.
DOI:10.1111/adj.12103 - ↑ Slavkin HC, «Research on Craniofacial Genetics and Developmental Biology: Implications for the Future of Academic Dentistry», in J Dent Educ, 1983.
PMID:6573384 - ↑ Slavkin HC, «The Future of Research in Craniofacial Biology and What This Will Mean for Oral Health Professional Education and Clinical Practice», in Aust Dent J, 2014.
PMID:24433547
DOI:10.1111/adj.12105 - ↑
Littlewood SJ, Kandasamy S, Huang G, «Retention and relapse in clinical practice», in Aust Dent J, 2017.
DOI:10.1111/adj.12475 - ↑ Miamoto CB, Silva Marques L, Abreu LG, Paiva SM, «Impact of two early treatment protocols for anterior dental crossbite on children’s quality of life», in Dental Press J Orthod, 2018.
- ↑ Alachioti XS, Dimopoulou E, Vlasakidou A, Athanasiou AE, «Amelogenesis imperfecta and anterior open bite: Etiological, classification, clinical and management interrelationships», in J Orthod Sci, 2014.
DOI:10.4103/2278-0203.127547 - ↑ Mizrahi E, «A review of anterior open bite», in Br J Orthod, 1978.
PMID:284793
DOI:10.1179/bjo.5.1.21 - ↑ Por uma questão de simplicidade de exposição e leitura, vamos lidar neste capítulo com o símbolo de pertença , o símbolo de consequência e o " tal que " como se fossem quantificadores e conectivos de proposições na lógica clássica.
A rigor, dentro da lógica clássica, eles não devem ser tratados como tal, mas mesmo que o façamos, isso não muda absolutamente o significado do discurso e nenhuma inconsistência de qualquer tipo é criada.. - ↑ Pereira LM, Pinto AM, «Reductio ad Absurdum Argumentation in Normal Logic Programs», Arg NMR, 2007, Tempe, Arizona - Caparica, Portugal – in Argumentation and Non-Monotonic Reasoning - An LPNMR Workshop.
- ↑ Castroflorio T, Talpone F, Deregibus A, Piancino MG, Bracco P, «Effects of a Functional Appliance on Masticatory Muscles of Young Adults Suffering From Muscle-Related Temporomandibular Disorder», in J Oral Rehabil, 2004.
PMID:15189308
DOI:10.1111/j.1365-2842.2004.01274.x - ↑ Maeda N, Kodama N, Manda Y, Kawakami S, Oki K, Minagi S, «Characteristics of Grouped Discharge Waveforms Observed in Long-term Masseter Muscle Electromyographic Recording: A Preliminary Study», in Acta Med Okayama, Okayama University Medical School, 2019, Okayama, Japan.
PMID:31439959
DOI:10.18926/AMO/56938 - ↑ Rudy TE, «Psychophysiological Assessment in Chronic Orofacial Pain», in Anesth Prog, American Dental Society of Anesthesiology, 1990.
ISSN: 0003-3006/90
PMID:2085203 - PMCID:PMC2190318 - ↑ Woźniak K, Piątkowska D, Lipski M, Mehr K, «Surface electromyography in orthodontics - a literature review», in Med Sci Monit, 2013.
e-ISSN: 1643-3750
PMID:23722255 - PMCID:PMC3673808
DOI:10.12659/MSM.883927 - ↑ Liang X, Liu S, Qu X, Wang Z, Zheng J, Xie X, Ma G, Zhang Z, Ma X, «Evaluation of Trabecular Structure Changes in Osteoarthritis of the Temporomandibular Joint With Cone Beam Computed Tomography Imaging», in Oral Surg Oral Med Oral Pathol Oral Radiol, 2017.
PMID:28732700
DOI:10.1016/j.oooo.2017.05.514 - ↑ Solberg WK, Bibb CA, Nordström BB, Hansson TL, «Malocclusion Associated With Temporomandibular Joint Changes in Young Adults at Autopsy», in Am J Orthod, 1986.
PMID:3457531
DOI:10.1016/0002-9416(86)90055-2 - ↑ KaVo Dental GmbH, Biberach / Ris
- ↑ Kobs G, Didziulyte A, Kirlys R, Stacevicius M, «Reliability of ARCUSdigma (KaVo) in Diagnosing Temporomandibular Joint Pathology», in Stomatologija, 2007.
PMID:17637527 - ↑ Piancino MG, Roberi L, Frongia G, Reverdito M, Slavicek R, Bracco P, «Computerized axiography in TMD patients before and after therapy with 'function generating bites'», in J Oral Rehabil, 2008.
PMID:18197841
DOI:10.1111/j.1365-2842.2007.01815.x - ↑ López-Cedrún J, Santana-Mora U, Pombo M, Pérez Del Palomar A, Alonso De la Peña V, Mora MJ, Santana U, «Jaw Biodynamic Data for 24 Patients With Chronic Unilateral Temporomandibular Disorder», in Sci Data, 2017.
PMID:29112190 - PMCID:PMC5674825
DOI:10.1038/sdata.2017.168

This is an Open Access resource - ↑ Myotronics Inc., Kent, WA, US
- ↑ Oliveira Mazzetto M, Almeida Rodrigues C, Valencise Magri L, Oliveira Melchior M, Paiva G, «Severity of TMD Related to Age, Sex and Electromyographic Analysis», in Braz Dent J, 2014.
DOI:10.1590/0103-6440201302310 - ↑ LeResche L, «Epidemiology of temporomandibular disorders: implications for the investigation of etiologic factors», in Crit Rev Oral Biol Med, 1997.
PMID:9260045
DOI:10.1177/10454411970080030401
particularly focusing on the field of the neurophysiology of the masticatory system