Difference between revisions of "The logic of classical language/it"
(Created page with "Cercando di utilizzare il formalismo matematico per tradurre le conclusioni raggiunte dal dentista con il linguaggio logico classico, consideriamo i seguenti predicati") |
(Created page with "Pazienti normali (normale sta per pazienti comunemente presenti in ambito specialistico)") |
||
| Line 581: | Line 581: | ||
Cercando di utilizzare il formalismo matematico per tradurre le conclusioni raggiunte dal dentista con il linguaggio logico classico, consideriamo i seguenti predicati: | Cercando di utilizzare il formalismo matematico per tradurre le conclusioni raggiunte dal dentista con il linguaggio logico classico, consideriamo i seguenti predicati: | ||
| − | *''x'' <math>\equiv</math> | + | *''x'' <math>\equiv</math> Pazienti normali (normale sta per pazienti comunemente presenti in ambito specialistico) |
*<math>A(x) \equiv</math> Bone remodelling with osteophyte from stratigraphic examination and condylar CT; e | *<math>A(x) \equiv</math> Bone remodelling with osteophyte from stratigraphic examination and condylar CT; e | ||
Revision as of 09:39, 2 November 2021

In conclusione, è evidente che una logica di linguaggio classica, che ha un approccio estremamente dicotomico (o qualcosa è bianco, o è nero), non può descrivere le molte sfumature che hanno le situazioni cliniche reali..
Come vedremo tra poco, questo articolo mostrerà che la logica classica manca della precisione necessaria, costringendoci a migliorarla con altri tipi di logica di linguaggio..
Introduzione
Ci siamo lasciati nel capitolo precedente sulla 'Logica del linguaggio medico nel tentativo di spostare l'attenzione dal sintomo o segno clinico al linguaggio macchina criptato per il quale, gli argomenti di Donald E Stanley, Daniel G Campos e Pat Croskerry sono benvenuti solo se legati al tempo come vettore di informazione (anticipazione del sintomo) e al messaggio come linguaggio macchina e non come linguaggio verbale).[1][2]
Ovviamente, questo non esclude la validità della storia clinica costruita su un linguaggio verbale pseudo-formale ormai ben radicato nella realtà clinica e che ha già dimostrato la sua autorità diagnostica. Il tentativo di spostare l'attenzione su un linguaggio macchina e sul Sistema non fornisce altro che un'opportunità per l'implementazione della Scienza Medica Diagnostica.

Siamo sicuramente consapevoli che il nostro Linux Sapiens è ancora perplesso su ciò che è stato anticipato e continua a chiedersi

(un po' di pazienza, per favore)
Non possiamo fornire una risposta convenzionale perché la scienza non progredisce con affermazioni che non sono giustificate da domande e riflessioni scientificamente validate; ed è proprio questo il motivo per cui cercheremo di dare voce ad alcuni pensieri, perplessità e dubbi espressi su alcuni argomenti fondamentali portati in discussione in alcuni articoli scientifici.
Uno di questi argomenti fondamentali è la "Biologia Craniofacciale"..
Cominciamo con uno studio ben noto di Townsend e Brook[3]: in questo lavoro gli autori considerano lo status quo della ricerca fondamentale e applicata in "Biologia Craniofacciale" per estrarre notevoli implicazioni cliniche. Un argomento che hanno trattato è stato l'"Approccio interdisciplinare", in cui Geoffrey Sperber e suo figlio Steven hanno visto la forza del progresso esponenziale della 'Biologia Craniofacciale' nelle innovazioni tecnologiche come il sequenziamento dei geni, la scansione CT, l'imaging MRI, la scansione laser, l'analisi delle immagini, l'ultrasonografia e la spettroscopia[4].
Un altro argomento di grande interesse per l'implementazione della 'Biologia Craniofacciale' è la consapevolezza che i sistemi biologici sono 'Sistemi Complessi'.[5] e che l'epigenetica gioca un ruolo chiave nella biologia molecolare craniofacciale. Ricercatori Australiani di Adelaide e Sydney forniscono una revisione critica nel campo dell'epigenetica rivolta, appunto, alle discipline dentali e craniofacciali.[6] La fenomica, in particolare, discussa da questi autori Phenomics)) è un campo di ricerca generale che coinvolge la misurazione dei cambiamenti nei denti e nelle strutture orofacciali associate derivanti dalle interazioni tra fattori genetici, epigenetici e ambientali durante lo sviluppo.[7] In questo stesso contesto, il lavoro di Irma Thesleff di Helsinki, Finlandia, dovrebbe essere evidenziato. Nel suo lavoro spiega che ci sono una serie di centri di segnalazione transitori nell'epitelio dentale che svolgono ruoli importanti nel programma di sviluppo dei denti.[8] Inoltre ci sono altri lavori, da Peterkova R, Hovor Akova M, Peterka M, Lesot H, che forniscono una revisione affascinante dei processi che si verificano durante lo sviluppo dentale;[9][10][11] per completezza, non dimentichiamo i lavori di Han J, Menicanin D, Gronthos S, e Bartold PM., che recensiscono la documentazione completa sulle cellule staminali, l'ingegneria dei tessuti e la rigenerazione parodontale.[12]
In questa rassegna, non potevano mancare argomenti sulle influenze genetiche, epigenetiche e ambientali durante la morfogenesi che portano a variazioni nel numero, dimensione e forma del dente[13][14] e l'influenza della pressione della lingua sulla crescita e la funzione cranio-facciale.[15][16]
Anche lo straordinario lavoro di Townsend e Brook merita una menzione[3], e il contenuto intrinseco di ciò che è stato riportato in esso corrisponde altrettanto bene ad un altro autore encomiabile: HC Slavkin.[17] Slavkin afferma che:
- "Il futuro è pieno di opportunità significative per migliorare i risultati clinici delle malformazioni craniofacciali congenite e acquisite. I clinici giocano un ruolo chiave in quanto il pensiero critico e migliorano sostanzialmente l'accuratezza diagnostica e quindi i risultati di salute clinica."
(Ti darò un esempio pratico)
Nel capitolo " "Introduction" abbiamo posto alcune domande sul tema della malocclusione ma in questo contesto simuliamo la logica del linguaggio medico del dentista di fronte al caso clinico presentato nel "capitolo Introduzione" con le sue conclusioni diagnostiche e terapeutiche.
Il paziente ha un crossbite unilaterale posteriore e un openbite anteriore.[18] Il crossbite è un altro elemento di disturbo dell'occlusione normale[19] per il quale è obbligatoriamente trattato insieme all'openbite.[20][21] Questo tipo di ragionamento significa che il modello (sistema masticatorio) è "normalizzato all'occlusione"; e letto al contrario, significa che la discrepanza occlusale è la causa della malocclusione, quindi, una malattia del Sistema Masticatorio, e quindi un intervento per ripristinare la funzione masticatoria fisiologica è giustificabile. (Figura 1a).
Questo esempio è il linguaggio logico classico, come spiegheremo in dettaglio, ma ora sorge un dubbio:
- All'epoca in cui gli assiomi dell'ortodonzia e dell'ortognatodonzia stavano costruendo protocolli confermati dalla Comunità Scientifica Internazionale, erano a conoscenza delle informazioni di cui abbiamo parlato nell'introduzione di questo capitolo?
Certamente che no, perché il tempo è il portatore di informazioni ma nonostante questo limite cognitivo si procede con una Logica del Linguaggio Classico molto discutibile per la sicurezza del paziente.
(certo, ma la sequenza logica è già stata anticipata)
Se lo stesso caso fosse interpretato con una mentalità che segue una "logica di linguaggio di sistema" (sarà discusso nel capitolo appropriato), le conclusioni sarebbero sorprendenti.
Se osserviamo le risposte elettrofisiologiche eseguite sul paziente con malocclusione nelle figure 1b, 1c e 1d (con la spiegazione fatta direttamente nella didascalia per semplificare la discussione), noteremo che questi dati possono farci pensare a tutto tranne che a una 'Malocclusione' e, quindi, gli assiomi di tipo ortodontico e ortognatico 'causa/effetto' lasciano un vuoto concettuale.

Figura 1a: Paziente con malocclusione, morso aperto e morso incrociato posteriore destro che in termini riabilitativi deve essere trattato con terapia ortodontica e/o chirurgia ortognatica
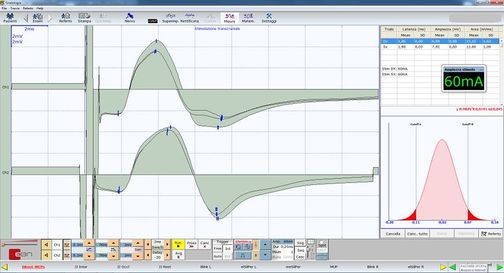
Figura 1b: Potenziale evocato motorio da stimolazione elettrica transcranica delle radici trigeminali. Si noti la simmetria strutturale calcolata dall'ampiezza picco-picco sui masseteri destro e sinistro (tracce in alto e in basso rispettivamente)
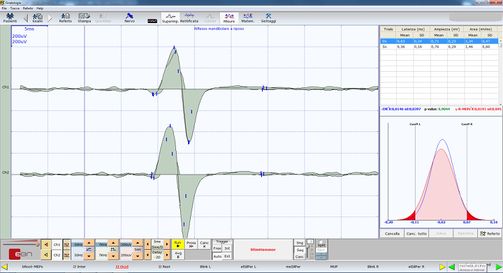
Figura 1c: Riflesso mandibolare evocato o jaw jerk da percussione del mento attraverso un martelletto neurologico triggerato . Si noti la simmetria funzionale calcolata dall'ampiezza picco-picco sui masseteri destro e sinistro (tracce superiori e inferiori rispettivamente)
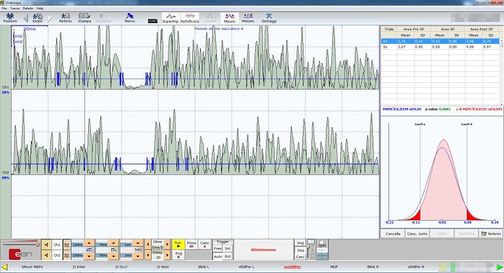
Figura 1d: Periodo di silenzio meccanico evocato dalla percussione del mento attraverso un martello neurologico triggerato. Si noti la simmetria funzionale calcolata sull'area integrale dei masseteri destro e sinistro (tracce superiori e inferiori rispettivamente).



(Lo faremo seguendo il caso clinico della nostra Mary Poppins)
Formalismo matematico
In questo capitolo, riconsidereremo il caso clinico della sfortunata Mary Poppins che soffriva di dolore orofacciale da più di 10 anni e alla quale il suo dentista diagnosticò un 'Disturbo Temporomandibolare' (DTM) o piuttosto un dolore orofacciale da DTM. Per capire meglio perché l'esatta formulazione diagnostica rimane complessa con una Logica del Linguaggio Classico, dovremmo capire il concetto su cui si basa la filosofia del linguaggio classico con una breve introduzione all'argomento.
Proposizioni
La logica classica si basa sulle proposizioni. Si dice spesso che una proposizione è una frase che chiede se la proposizione è vera o falsa. Infatti, una proposizione in matematica è di solito o vera o falsa, ma questo è ovviamente un po' troppo vago per essere una definizione. Può essere preso, al massimo, come un avvertimento: se una frase, espressa nel linguaggio comune, non ha senso chiedere se è vera o falsa, non sarà una proposizione ma qualcos'altro.
Si può discutere se le frasi del linguaggio comune siano o meno proposizioni, poiché in molti casi non è spesso evidente se una certa affermazione sia vera o falsa.
‘Fortunatamente, le proposizioni matematiche, se ben espresse, non mostrano tali ambiguità’.
Le proposizioni più semplici possono essere combinate tra loro per formare nuove proposizioni più complesse. Questo avviene con l'aiuto di operatori chiamati operatori logici e connettivi quantificatori che possono essere ridotti ai seguenti[22]:
- Congiunzione, che è indicata dal simbolo (and):
- Disgiunzione, che è indicata dal simbolo (or):
- Negazione, che è indicata dal simbolo (not):
- Implicazione, che è indicata dal simbolo (if ... then):
- Consequence, che è indicata dal simbolo (is a partition of..):
- Quantificatore universale, che è indicata dal simbolo (for all):
- Dimostrazione, che è indicata dal simbolo (such that): and
- Appartenenza, che è indicata dal simbolo (is an element of) o dal simbolo (is not an element of):









Dimostrazione per assurdo
Inoltre, nella logica classica c'è un principio chiamato il terzo escluso che dichiara che una frase che non può essere falsa deve essere presa come vera poiché non c'è una terza possibilità.
Supponiamo di dover dimostrare che la proposizione è vera. Il procedimento consiste nel mostrare che l'assunzione che sia falsa porta a una contraddizione logica. Così la proposizione non può essere falsa, e quindi, secondo la legge del terzo escluso, deve essere vera. Questo metodo di dimostrazione è chiamato dimostrazione per assurdo.[23]

Predicati
Quella che abbiamo descritto brevemente finora è la logica delle proposizioni. Una proposizione afferma qualcosa su specifici oggetti matematici come: '2 è maggiore di 1, quindi 1 è minore di 2' o 'un quadrato non ha 5 lati quindi un quadrato non è un pentagono'.. Molte volte, però, le affermazioni matematiche non riguardano il singolo oggetto, ma oggetti generici di un insieme come: ' sono più alti di 2 metri' dove denota un gruppo generico (per esempio tutti i giocatori di pallavolo). In questo caso si parla di predicati.

Intuitivamente, un predicato è una frase che riguarda un gruppo di elementi (che nel nostro caso medico saranno i pazienti) e che afferma qualcosa su di loro.
(vediamo cosa ci dice la logica di linguaggio classica)
Oltre alle conferme derivate dalla logica del linguaggio medico discusse nel capitolo precedente, il collega dentista acquisisce altri dati strumentali che gli permettono di confermare la sua diagnosi. Queste ultime prove riguardano l'analisi dei tracciati assiografici attraverso l'utilizzo di un cucchiaio paraocclusale funzionale personalizzato che permette la visualizzazione e la quantificazione dei tracciati condilari nelle funzioni masticatorie. Come si può vedere dalla Figura 4 l'appiattimento del tracciato condilari sul lato destro sia nella cinetica masticatoria mediotrusiva (colore verde) che nei cicli di apertura e protrusione (colore grigio) confermano l'appiattimento anatomico e funzionale dell'ATM destra nella masticazione dinamica. Oltre all'assiografia, il collega esegue un'elettromiografia di superficie sui masseteri (Fig. 6) chiedendo al paziente di esercitare la massima forza dei suoi muscoli. Questo tipo di analisi elettromiografica è chiamato "EMG Interferential Pattern" a causa del contenuto di alta frequenza dei picchi che subiscono una interferenze di fase. Infatti, la figura 6 mostra un'asimmetria nel reclutamento delle unità motorie del massetere destro (traccia superiore) rispetto a quelle del massetere sinistro (traccia inferiore).[24][25][26][27]
Secondo approccio clinico
(passa il mouse sulle immagini)

Figura 2: Paziente che riferisce 'Dolore orofacciale' nell'emilato destro della faccia

Figura 3: La stratigrafia dell'ATM del paziente mostra segni di appiattimento condilare e osteofita

Figura 4: Tomografia computerizzata dell'ATM
Figura 5: Assiografia del paziente che mostra un appiattimento del modello di masticazione sul condilo destro
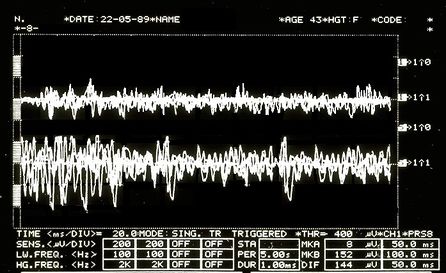
Figura 6: Modello interferenziale EMG. Tracce superiori sovrapposte corrispondenti al massetere destro, inferiori al massetere sinistro.




Proposizioni odontoiatriche
Cercando di utilizzare il formalismo matematico per tradurre le conclusioni raggiunte dal dentista con il linguaggio logico classico, consideriamo i seguenti predicati:
- x Pazienti normali (normale sta per pazienti comunemente presenti in ambito specialistico)

- Bone remodelling with osteophyte from stratigraphic examination and condylar CT; e
- Temporomandibular Disorders (TMDs) resulting in Orofacial Pain (OP)
- Specific patient: Mary Poppins



Any normal patient who is positive on the radiographic examination of the TMJ [Figura 2 e 3] is affected by TMDs ; from this it follows that being Mary Poppins positive (and also being a "Normal" patient) on the TMJ x-ray then Mary Poppins is also affected by TMDs





The language of predicates is expressed in the following way:
.


At this point, it must also be considered that predicate logic is not used only to prove that a particular set of premises imply a particular evidence . It is also used to prove that a particular assertion is not true, or that a particular piece of knowledge is logically compatible/incompatible with a particular evidence.
In order to prove that this proposition is true we must use the above mentioneddimostrazione per assurdo. If its denial creates a contradiction, surely the dentist's proposition will be true:
.


"" states that it is not true that those who test positive on TMJ CT have TMDs, so Mary Poppins (TMJ CT positive normal patient) does not have TMDs.
The dentist believes that Mary Poppins' claim (that she does not have TMD under these premises) is a contradiction so the main claim is true.
Neurophysiological proposition
Let us imagine that the neurologist disagrees with the conclusion e asserts that Mary Poppins is not affected by TMDs or that at least it is not the main cause of Orofacial Pain, but that, rather, she is affected by a neuromotor Orofacial Pain (nOP), therefore that she does not belong to the group of 'normal patients' but is to be considered a 'non-specific patient' (uncommon in the specialist context).
Obviously, this dialectic would last indefinitely because both would defend their scientific-clinical context; but let us see what happens in the logic of predicates.
The neurologist's statement would be like:
.


"" means that every patient who is TMJ CT positive has TMDs but even though Mary Poppins is TMJ CT positive, she does not have TMDs.
In order to prove that this proposition is true, we must use once again the above mentioned dimostrazione per assurdo. If its denial creates a contradiction, surely the neurologist's proposition will be true:
.


Following the logical rules of predicates, there is no reason to say that denial (4) is contradictory or meaningless, therefore the neurologist (unlike the dentist) would not seem to have the logical tools to confirm his conclusion.
(non darlo per scontato)
Compatibility and incompatibility of the statements
The complication lies in the fact that the dentist will present a series of statements as clinical reports such as the stratigraphy and CT of the TMJ, that indicate an anatomical flattening of the joint, axiography of the condylar traces with a reduction in kinematic convexity and a tracing EMG interference pattern in which an asymmetrical pattern on the masseters is highlighted. These assertions can easily be considered a contributing cause of the damage to the Temporomandibular Joint and, therefore, responsible for the 'Orofacial pain'.
Documents, reports and clinical evidence can be used to make the neurologist's assertion incompatible and the dentist's diagnostic conclusion compatible. To do this we must present some logical rules that describe the compatibility or incompatibility of the logic of classical language:
- A set of sentences , e a number of other phrases or statements are logically compatible if, and only if, the union between them is coherent.
- A set of sentences , e a number of other phrases or statements are logically incompatible if, and only if, the union between them is incoherent.




Let us try to follow this reasoning with practical examples:
The dentist colleague exposes the following sentence:
: Following the personalized techniques suggested by Xin Liang et al.[28] who focuses on the quantitative microstructural analysis of the fraction of the bone value, the trabecular number, the trabecular thickness and the trabecular separation on each slice of the CT scan of a TMJ, it appears that Mary Poppins is affected by Temporomandibular Disorders (TMDs) and the consequence causes Orofacial Pain.
At this point, however, the thesis must be confirmed with further clinical and laboratory tests, and in fact the colleague produces a series of assertions that should pass the compatibility filter as described above, namely:
Bone remodelling: The flattening of the axiographic traces highlighted in figure 5 indicates the joint remodelling of the right TMJ of Mary Poppins, such a report can be correlated to a series of researches and articles that confirm how malocclusion can be associated with morphological changes in the temporomandibular joints, particularly when combined with the age as the presence of a chronic malocclusion can worsen the picture of bone remodelling.[29] These scientific references determine the compatibility of the assertion.

Sensitivity and specificity of the axiographic measurement: A study was conducted to verify the sensitivity and specificity of the data collected from a group of patients affected by temporomandibular joint disorders with an ARCUSdigma axiographic system[30]; it confirmed a sensitivity of the 84.21% and a 92.86% sensitivity for the right and left TMJs respectively, and a specificity of 93.75% and 95.65%.[31] These scientific references determine compatibility of the assertion in the dental context precisely because of the consistency of related studies.[32]

Alteration of condylar paths: Urbano Santana-Mora e coll.[33] evaluated 24 adult patients suffering from severe chronic unilateral pain diagnosed as Temporomandibular Disorders (TMDs). The following functional and dynamic factors were evaluated:

- masticatory function;
- remodelling of the TMJ or condylar pathway (CP); e
- lateral movement of the jaw or lateral guide (LG).
The CPs were assessed using conventional axiography and LG was assessed by using kinesiograph tracing[34]; Seventeen (71%) of the 24 (100%) patients consistently showed a side of habitual chewing side. The mean and standard deviation of the CP angles was 47.90 9.24) gradi. The average of LG angles was 42.9511.78 gradi.
Data collection emerged from the conception of a new TMD paradigm in which the affected side could be the usual chewing side, the side where the mandibular lateral kinematic angle was flatter. This parameter may also be compatible with the dental claim.

EMG Intereference pattern: M.O. Mazzetto e coll.[35] showed that the electromyographic activity of the anterior temporal muscles and the masseter was positively correlated with the "Craniomandibular index", indiced (CMI) with a and suggesting that the use of CMI to quantify the severity of TMDs and EMG to assess the masticatory muscle function, may be an important diagnostic and therapeutic elements. These scientific references determine compatibility of the assertion.


?

Obviously, the dentist colleague could endlessly keep on casting his statements, indefinitely.
Bene, all of these statements seem coherent with the sentence initially described, whereby the dentist colleague feels justified in saying that the set of sentences , and a number of other assertions or clinical data are logically compatible as the union between them is coherent.
(It would seem so!
But, be careful, only in his own dental context!)
This statement is so true that the could be infinitely extended, widened enough to obtain an that corresponds to it in an infinite significance, as long as it remains limited in its context; yet, without meaning anything from a clinical point of view in other contexts, like in the neurologist one, for instance.


Considerazioni finali
From a perspective of observation of this kind, the Logic of Predicates can only fortify the dentist’s reasoning and, at the same time, strengthen the principio del terzo escluso: the principle is strengthened through the compatibility of the additional assertions which grant the dentist a complete coherence in the diagnosis and in confirming the sentence : Poor Mary Poppins either has TMD, or she has not.
Basically, given the compatibility of the assertions , coherently saying that Orofacial Pain is caused by a Temporomandibular Disorders could become incompatible if another series of assertions were shown to be coherent: this would make a different sentence compatible : could poor Mary Poppins suffer from Orofacial Pain from a neuromotor disorder (nOP) and not by a Temporomandibular Disorders?

In the current medical language logic, such assertions only remain assertions, because the convictions and opinions do not allow a consequent and quick change of the mindset.
Moreover, taking into account the risk that this change entails, in fact, we might consider a recent article on the epidemiology of temporomandibular disorders[36] in which the authors confirm that despite the methodological and population differences, pain in the temporomandibular region appears to be relatively common, occurring in about the 10% of the population; we may then objectively be led to hypothesize that our Mary Poppins can be included in the 10% of the patients mentioned in the epidemiological study, and contextually be classified as a patient suffering from Orofacial Pain from Temporomandibular Disorders (TMDs).
In conclusion, it is evident that a classical logic of language, which has an extremely dichotomous approach (either it is white or it is black), cannot depict the many shades that occur in real clinical situations.
We need to find a more convenient and suitable language logic...
(forse)
- ↑ Stanley DE, Campos DG, «The logic of medical diagnosis», in Perspect Biol Med, 2013.
PMID:23974509
DOI:10.1353/pbm.2013.0019 - ↑ Croskerry P, «Adaptive expertise in medical decision making», in Med Teach, 2018.
PMID:30033794
DOI:10.1080/0142159X.2018.1484898 - ↑ 3.0 3.1 Townsend GC, Brook AH, «The face, the future, and dental practice: how research in craniofacial biology will influence patient care», in Aust Dent J, Australian Dental Association, 2014.
PMID:24646132
DOI:10.1111/adj.12157 - ↑ Sperber GH, Sperber SM, «The genesis of craniofacial biology as a health science discipline», in Aust Dent J, Australian Dental Association, 2014.
PMID:24495071
DOI:10.1111/adj.12131 - ↑ Brook AH, Brook O'Donnell M, Hone A, Hart E, Hughes TE, Smith RN, Townsend GC, «General and craniofacial development are complex adaptive processes influenced by diversity», in Aust Dent J, Australian Dental Association, 2014.
PMID:24617813
DOI:10.1111/adj.12158 - ↑ Williams SD, Hughes TE, Adler CJ, Brook AH, Townsend GC, «Epigenetics: a new frontier in dentistry», in Aust Dent J, Australian Dental Association, 2014.
PMID:24611746
DOI:10.1111/adj.12155 - ↑ Yong R, Ranjitkar S, Townsend GC, Brook AH, Smith RN, Evans AR, Hughes TE, Lekkas D, «Dental phenomics: advancing genotype to phenotype correlations in craniofacial research», in Aust Dent J, Australian Dental Association, 2014.
PMID:24611797
DOI:10.1111/adj.12156 - ↑ Thesleff I, «Current understanding of the process of tooth formation: transfer from the laboratory to the clinic», in Aust Dent J, 2013.
DOI:10.1111/adj.12102 - ↑ Peterkova R, Hovorakova M, Peterka M, Lesot H, «Three‐dimensional analysis of the early development of the dentition», in Aust Dent J, Wiley Publishing Asia Pty Ltd on behalf of Australian Dental Association, 2014.
DOI:10.1111/adj.12130 - ↑ Lesot H, Hovorakova M, Peterka M, Peterkova R, «Three‐dimensional analysis of molar development in the mouse from the cap to bell stage», in Aust Dent J, 2014.
DOI:10.1111/adj.12132 - ↑ Hughes TE, Townsend GC, Pinkerton SK, Bockmann MR, Seow WK, Brook AH, Richards LC, Mihailidis S, Ranjitkar S, Lekkas D, «The teeth and faces of twins: providing insights into dentofacial development and oral health for practising oral health professionals», in Aust Dent J, 2013.
DOI:10.1111/adj.12101 - ↑ Han J, Menicanin D, Gronthos S, Bartold PM, «Stem cells, tissue engineering and periodontal regeneration», in Aust Dent J, 2013.
DOI:10.1111/adj.12100 - ↑ {{Cite book | autore = Brook AH | autore2 = Jernvall J | autore3 = Smith RN | autore4 = Hughes TE | autore5 = Townsend GC | titolo = The Dentition: The Outcomes of Morphogenesis Leading to Variations of Tooth Number, Size and Shape | url = https://onlinelibrary.wiley.com/doi/epdf/10.1111/adj.12160 | volume = | opera = Aust Dent J | anno = 2014 | editore = | città = | ISBN = | PMID = | PMCID = | DOI = 10.1111/adj.12160 | oaf = | LCCN = | OCLC =
- ↑ Seow WK, «Developmental defects of enamel and dentine: challenges for basic science research and clinical management», in Aust Dent J, 2014.
PMID:24164394
DOI:10.1111/adj.12104 - ↑ Kieser JA, Farland MG, Jack H, Farella M, Wang Y, Rohrle O, «The role of oral soft tissues in swallowing function: what can tongue pressure tell us?», in Aust Dent J, 2013.
DOI:10.1111/adj.12103 - ↑ Slavkin HC, «Research on Craniofacial Genetics and Developmental Biology: Implications for the Future of Academic Dentistry», in J Dent Educ, 1983.
PMID:6573384 - ↑ Slavkin HC, «The Future of Research in Craniofacial Biology and What This Will Mean for Oral Health Professional Education and Clinical Practice», in Aust Dent J, 2014.
PMID:24433547
DOI:10.1111/adj.12105 - ↑
Littlewood SJ, Kandasamy S, Huang G, «Retention and relapse in clinical practice», in Aust Dent J, 2017.
DOI:10.1111/adj.12475 - ↑ Miamoto CB, Silva Marques L, Abreu LG, Paiva SM, «Impact of two early treatment protocols for anterior dental crossbite on children’s quality of life», in Dental Press J Orthod, 2018.
- ↑ Alachioti XS, Dimopoulou E, Vlasakidou A, Athanasiou AE, «Amelogenesis imperfecta and anterior open bite: Etiological, classification, clinical and management interrelationships», in J Orthod Sci, 2014.
DOI:10.4103/2278-0203.127547 - ↑ Mizrahi E, «A review of anterior open bite», in Br J Orthod, 1978.
PMID:284793
DOI:10.1179/bjo.5.1.21 - ↑ Per semplicità di esposizione e di lettura, tratteremo in questo capitolo il simbolo di appartenenza, il simbolo di conseguenza e il tale che come se fossero quantificatori e connettivi di proposizioni nella logica classica.
In senso stretto, all'interno della logica classica non dovrebbero essere trattati come tali, ma anche se lo facciamo, questo non cambia assolutamente il significato del discorso e non si creano incongruenze di nessun tipo. - ↑ Pereira LM, Pinto AM, «Reductio ad Absurdum Argumentation in Normal Logic Programs», Arg NMR, 2007, Tempe, Arizona - Caparica, Portugal – in Argumentation and Non-Monotonic Reasoning - An LPNMR Workshop.
- ↑ Castroflorio T, Talpone F, Deregibus A, Piancino MG, Bracco P, «Effects of a Functional Appliance on Masticatory Muscles of Young Adults Suffering From Muscle-Related Temporomandibular Disorder», in J Oral Rehabil, 2004.
PMID:15189308
DOI:10.1111/j.1365-2842.2004.01274.x - ↑ Maeda N, Kodama N, Manda Y, Kawakami S, Oki K, Minagi S, «Characteristics of Grouped Discharge Waveforms Observed in Long-term Masseter Muscle Electromyographic Recording: A Preliminary Study», in Acta Med Okayama, Okayama University Medical School, 2019, Okayama, Japan.
PMID:31439959
DOI:10.18926/AMO/56938 - ↑ Rudy TE, «Psychophysiological Assessment in Chronic Orofacial Pain», in Anesth Prog, American Dental Society of Anesthesiology, 1990.
ISSN: 0003-3006/90
PMID:2085203 - PMCID:PMC2190318 - ↑ Woźniak K, Piątkowska D, Lipski M, Mehr K, «Surface electromyography in orthodontics - a literature review», in Med Sci Monit, 2013.
e-ISSN: 1643-3750
PMID:23722255 - PMCID:PMC3673808
DOI:10.12659/MSM.883927 - ↑ Liang X, Liu S, Qu X, Wang Z, Zheng J, Xie X, Ma G, Zhang Z, Ma X, «Evaluation of Trabecular Structure Changes in Osteoarthritis of the Temporomandibular Joint With Cone Beam Computed Tomography Imaging», in Oral Surg Oral Med Oral Pathol Oral Radiol, 2017.
PMID:28732700
DOI:10.1016/j.oooo.2017.05.514 - ↑ Solberg WK, Bibb CA, Nordström BB, Hansson TL, «Malocclusion Associated With Temporomandibular Joint Changes in Young Adults at Autopsy», in Am J Orthod, 1986.
PMID:3457531
DOI:10.1016/0002-9416(86)90055-2 - ↑ KaVo Dental GmbH, Biberach / Ris
- ↑ Kobs G, Didziulyte A, Kirlys R, Stacevicius M, «Reliability of ARCUSdigma (KaVo) in Diagnosing Temporomandibular Joint Pathology», in Stomatologija, 2007.
PMID:17637527 - ↑ Piancino MG, Roberi L, Frongia G, Reverdito M, Slavicek R, Bracco P, «Computerized axiography in TMD patients before and after therapy with 'function generating bites'», in J Oral Rehabil, 2008.
PMID:18197841
DOI:10.1111/j.1365-2842.2007.01815.x - ↑ López-Cedrún J, Santana-Mora U, Pombo M, Pérez Del Palomar A, Alonso De la Peña V, Mora MJ, Santana U, «Jaw Biodynamic Data for 24 Patients With Chronic Unilateral Temporomandibular Disorder», in Sci Data, 2017.
PMID:29112190 - PMCID:PMC5674825
DOI:10.1038/sdata.2017.168

This is an Open Access resource - ↑ Myotronics Inc., Kent, WA, US
- ↑ Oliveira Mazzetto M, Almeida Rodrigues C, Valencise Magri L, Oliveira Melchior M, Paiva G, «Severity of TMD Related to Age, Sex and Electromyographic Analysis», in Braz Dent J, 2014.
DOI:10.1590/0103-6440201302310 - ↑ LeResche L, «Epidemiology of temporomandibular disorders: implications for the investigation of etiologic factors», in Crit Rev Oral Biol Med, 1997.
PMID:9260045
DOI:10.1177/10454411970080030401
particularly focusing on the field of the neurophysiology of the masticatory system